
Page 133 - Biomedical Engineering and Design Handbook Volume 2, Applications
P. 133
112 MEDICAL DEVICE DESIGN
blood to participate in gas exchange. The network of alveoli and airways is interdependent, so that
the walls of the alveoli are shared among neighboring lung units.
Inspiration of fresh air occurs when respiratory muscles, chiefly the diaphragm, contract, expand-
ing the chest wall and decreasing slightly the pressure surrounding the lungs but within the chest cav-
ity (the pleural pressure). This drop in pleural pressure tends to pull outward on the outer lung
surfaces, which in turn pull outward on more central lung units due to interdependence, and so on,
with the result that the pressure within the alveolar air spaces falls. When alveolar pressure falls
below the surrounding atmospheric pressure, air flows down the pressure gradient, filling the alveoli
with inspired gas. Because lung tissue is elastic, it will tend to deflate when inspiratory muscle forces
are released. In a normal person at rest, expiration is a passive phase and requires no muscular
activity.
If all of a person’s muscles were paralyzed and the lung was then permitted to empty, the lung
volume would decrease to the functional residual capacity (FRC). At this volume, lung elasticity
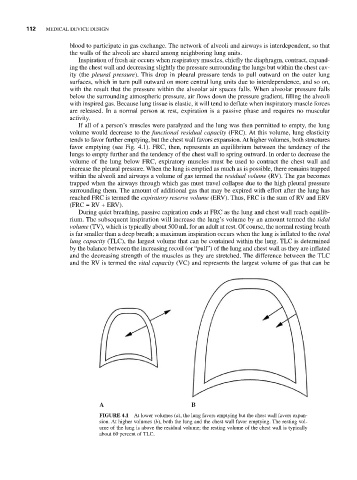
tends to favor further emptying, but the chest wall favors expansion. At higher volumes, both structures
favor emptying (see Fig. 4.1). FRC, then, represents an equilibrium between the tendency of the
lungs to empty further and the tendency of the chest wall to spring outward. In order to decrease the
volume of the lung below FRC, expiratory muscles must be used to contract the chest wall and
increase the pleural pressure. When the lung is emptied as much as is possible, there remains trapped
within the alveoli and airways a volume of gas termed the residual volume (RV). The gas becomes
trapped when the airways through which gas must travel collapse due to the high pleural pressure
surrounding them. The amount of additional gas that may be expired with effort after the lung has
reached FRC is termed the expiratory reserve volume (ERV). Thus, FRC is the sum of RV and ERV
(FRC = RV + ERV).
During quiet breathing, passive expiration ends at FRC as the lung and chest wall reach equilib-
rium. The subsequent inspiration will increase the lung’s volume by an amount termed the tidal
volume (TV), which is typically about 500 mL for an adult at rest. Of course, the normal resting breath
is far smaller than a deep breath; a maximum inspiration occurs when the lung is inflated to the total
lung capacity (TLC), the largest volume that can be contained within the lung. TLC is determined
by the balance between the increasing recoil (or “pull”) of the lung and chest wall as they are inflated
and the decreasing strength of the muscles as they are stretched. The difference between the TLC
and the RV is termed the vital capacity (VC) and represents the largest volume of gas that can be
A B
FIGURE 4.1 At lower volumes (a), the lung favors emptying but the chest wall favors expan-
sion. At higher volumes (b), both the lung and the chest wall favor emptying. The resting vol-
ume of the lung is above the residual volume; the resting volume of the chest wall is typically
about 60 percent of TLC.