
Page 74 - Mechatronics for Safety, Security and Dependability in a New Era
P. 74
Ch13-I044963.fm Page 58 Tuesday, August 1, 2006 12:49 PM
Ch13-I044963.fm
58 58 Page 58 Tuesday, August 1,2006 12:49 PM
Monitor
Rotation around 4.
the Axis : ] DOF
Surgeon Abdominal Wall
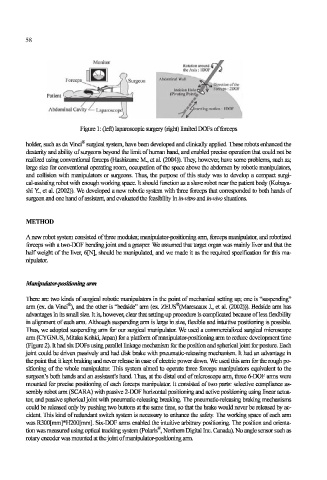
Figure 1: (left) laparoscopic surgery (right) limited DOFs of forceps
holder, such as da Vinci* surgical system, have been developed and clinically applied. These robots enhanced the
dexterity and ability of surgeons beyond the limit of human hand, and enabled precise operation that could not be
realized using conventional forceps (Hashizume M., et al. (2004)). They, however, have some problems, such as;
large size for conventional operating room, occupation of the space above the abdomen by robotic manipulators,
and collision with manipulators or surgeons. Thus, the purpose of this study was to develop a compact surgi-
cal-assisting robot with enough working space. It should function as a slave robot near the patient body (Kobaya-
shi Y., et al. (2002)). We developed a new robotic system with three forceps that corresponded to both hands of
surgeon and one hand of assistant, and evaluated the feasibility in in-vitro and in-vivo situations.
METHOD
Anew robot system consisted of three modules; manipulator-positioning arm, forceps manipulator, and robotized
forceps with a two-DOF bending joint and a grasper. We assumed that target organ was mainly liver and that the
half weight of the liver, 6[N], should be manipulated, and we made it as the required specification for this ma-
nipulator.
Manipulator-positioning arm
There are two kinds of surgical robotic manipulators in the point of mechanical setting up; one is "suspending"
I
arm (ex. da Vinci®), and the other is "bedside" arm (ex. ZEUS®(Marescaux , et al. (2002))). Bedside arm has
advantages in its small size. It is, however, clear that setting-up procedure is complicated because of less flexibility
in alignment of each arm. Although suspending arm is large in size, flexible and intuitive positioning is possible.
Thus, we adopted suspending arm for our surgical manipulator. We used a commercialized surgical microscope
arm (CYGNUS, Mitaka Kohki, Japan) for a platform of manipulator-positioning arm to reduce development time
(Figure 2). It had six DOFs using parallel linkage mechanism for the position and spherical joint for posture. Each
joint could be driven passively and had disk brake with pneumatic-releasing mechanism. It had an advantage in
the point that it kept braking and never release in case of electric power down. We used this arm for the rough po-
sitioning of the whole manipulator. This system aimed to operate three forceps manipulators equivalent to the
surgeon's both hands and an assistant's hand. Thus, at the distal end of microscope arm, three 6-DOF arms were
mounted for precise positioning of each forceps manipulator. It consisted of two parts: selective compliance as-
sembly robot arm (SCARA) with passive 2-DOF horizontal positioning and active positioning using linear actua-
tor, and passive spherical joint with pneumatic-releasing breaking. The pneumatic-releasing braking mechanisms
could be released only by pushing two buttons at the same time, so that the brake would never be released by ac-
cident. This kind of redundant switch system is necessary to enhance the safety. The working space of each arm
was R300[mm]*H200[mm]. Six-DOF arms enabled the intuitive arbitrary positioning. The position and orienta-
tion was measured using optical tacking system (Polaris®, Northern Digital Inc. Canada). No angle sensor such as
rotary encoder was mounted at the joint of manipulator-positioning arm.