
Page 159 - Urban Construction Project Management
P. 159
114 Chapter Five
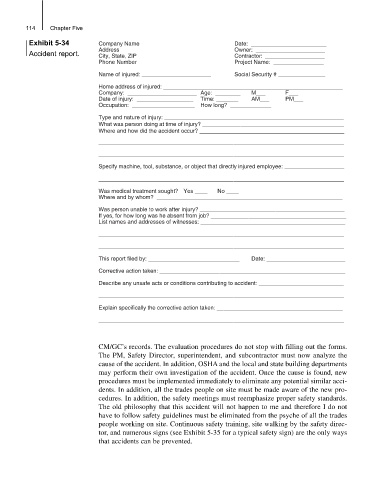
Exhibit 5-34 Company Name Date: ________________________
Address Owner: ______________________
Accident report. City, State, ZIP Contractor: ___________________
Phone Number Project Name: ________________
Name of injured: ______________________ Social Security # _______________
Home address of injured: _________________________________________________________
Company: ______________________ Age: ________ M___ F___
Date of injury: __________________ Time: _______ AM___ PM___
Occupation: ____________________ How long? _____________
Type and nature of injury: _________________________________________________________
What was person doing at time of injury? _____________________________________________
Where and how did the accident occur? ______________________________________________
______________________________________________________________________________
______________________________________________________________________________
Specify machine, tool, substance, or object that directly injured employee: ___________________
______________________________________________________________________________
Was medical treatment sought? Yes ____ No ____
Where and by whom? ___________________________________________________________
Was person unable to work after injury? ______________________________________________
If yes, for how long was he absent from job? ___________________________________________
List names and addresses of witnesses: ______________________________________________
______________________________________________________________________________
______________________________________________________________________________
This report filed by: _____________________________ Date: _________________________
Corrective action taken: ___________________________________________________________
Describe any unsafe acts or conditions contributing to accident: ___________________________
______________________________________________________________________________
Explain specifically the corrective action taken: ________________________________________
______________________________________________________________________________
CM/GC’s records. The evaluation procedures do not stop with filling out the forms.
The PM, Safety Director, superintendent, and subcontractor must now analyze the
cause of the accident. In addition, OSHA and the local and state building departments
may perform their own investigation of the accident. Once the cause is found, new
procedures must be implemented immediately to eliminate any potential similar acci-
dents. In addition, all the trades people on site must be made aware of the new pro-
cedures. In addition, the safety meetings must reemphasize proper safety standards.
The old philosophy that this accident will not happen to me and therefore I do not
have to follow safety guidelines must be eliminated from the psyche of all the trades
people working on site. Continuous safety training, site walking by the safety direc-
tor, and numerous signs (see Exhibit 5-35 for a typical safety sign) are the only ways
that accidents can be prevented.