
Page 381 - Biomedical Engineering and Design Handbook Volume 1, Fundamentals
P. 381
358 BIOMATERIALS
Type 4 (resorbable)
A
Type 3
Relative bioreactivity A bioactive Type 2
C
B
D porous ingrowth Type 1
F
nearly inert
E G
100 B
Percentage of interfacial bone tissue 60 A B A. 45SS bioglass
80
Bioceramics
B. KGS ceravital
C. 55S4.3 bioglass
40
D. A-W glass ceramic
E. Hydroxylapatite (HA)
20
O , Si N
G. Al 2 3
3 4
C D F. KGX ceravital
E F G
0
3 10 100 1000
Implantation time (days)
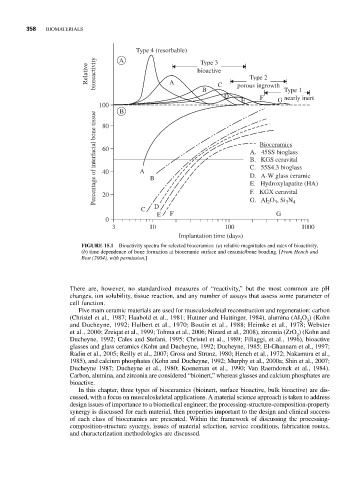
FIGURE 15.1 Bioactivity spectra for selected bioceramics: (a) relative magnitudes and rates of bioactivity,
(b) time dependence of bone formation at bioceramic surface and ceramic/bone bonding. [From Hench and
Best (2004), with permission.]
There are, however, no standardized measures of “reactivity,” but the most common are pH
changes, ion solubility, tissue reaction, and any number of assays that assess some parameter of
cell function.
Five main ceramic materials are used for musculoskeletal reconstruction and regeneration: carbon
(Christel et al., 1987; Haubold et al., 1981; Huttner and Huttinger, 1984), alumina (Al O ) (Kohn
2 3
and Ducheyne, 1992; Hulbert et al., 1970; Boutin et al., 1988; Heimke et al., 1978; Webster
et al., 2000; Zreiqat et al., 1999; Tohma et al., 2006; Nizard et al., 2008), zirconia (ZrO ) (Kohn and
2
Ducheyne, 1992; Cales and Stefani, 1995; Christel et al., 1989; Filiaggi, et al., 1996), bioactive
glasses and glass ceramics (Kohn and Ducheyne, 1992; Ducheyne, 1985; El-Ghannam et al., 1997;
Radin et al., 2005; Reilly et al., 2007; Gross and Strunz, 1980; Hench et al., 1972; Nakamura et al.,
1985), and calcium phosphates (Kohn and Ducheyne, 1992; Murphy et al., 2000a; Shin et al., 2007;
Ducheyne 1987; Ducheyne et al., 1980; Koeneman et al., 1990; Van Raemdonck et al., 1984).
Carbon, alumina, and zirconia are considered “bioinert,” whereas glasses and calcium phosphates are
bioactive.
In this chapter, three types of bioceramics (bioinert, surface bioactive, bulk bioactive) are dis-
cussed, with a focus on musculoskeletal applications. A material science approach is taken to address
design issues of importance to a biomedical engineer; the processing-structure-composition-property
synergy is discussed for each material, then properties important to the design and clinical success
of each class of bioceramics are presented. Within the framework of discussing the processing-
composition-structure synergy, issues of material selection, service conditions, fabrication routes,
and characterization methodologies are discussed.