
Page 100 - Biomedical Engineering and Design Handbook Volume 2, Applications
P. 100
OVERVIEW OF CARDIOVASCULAR DEVICES 79
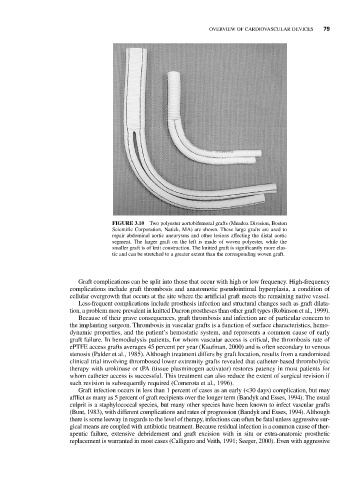
FIGURE 3.10 Two polyester aortobifemoral grafts (Meadox Division, Boston
Scientific Corporation, Natick, MA) are shown. These large grafts are used to
repair abdominal aortic aneurysms and other lesions affecting the distal aortic
segment. The larger graft on the left is made of woven polyester, while the
smaller graft is of knit construction. The knitted graft is significantly more elas-
tic and can be stretched to a greater extent than the corresponding woven graft.
Graft complications can be split into those that occur with high or low frequency. High-frequency
complications include graft thrombosis and anastomotic pseudointimal hyperplasia, a condition of
cellular overgrowth that occurs at the site where the artificial graft meets the remaining native vessel.
Less-frequent complications include prosthesis infection and structural changes such as graft dilata-
tion, a problem more prevalent in knitted Dacron prostheses than other graft types (Robinson et al., 1999).
Because of their grave consequences, graft thrombosis and infection are of particular concern to
the implanting surgeon. Thrombosis in vascular grafts is a function of surface characteristics, hemo-
dynamic properties, and the patient’s hemostatic system, and represents a common cause of early
graft failure. In hemodialysis patients, for whom vascular access is critical, the thrombosis rate of
ePTFE access grafts averages 45 percent per year (Kaufman, 2000) and is often secondary to venous
stenosis (Palder et al., 1985). Although treatment differs by graft location, results from a randomized
clinical trial involving thrombosed lower extremity grafts revealed that catheter-based thrombolytic
therapy with urokinase or tPA (tissue plasminogen activator) restores patency in most patients for
whom catheter access is successful. This treatment can also reduce the extent of surgical revision if
such revision is subsequently required (Comerota et al., 1996).
Graft infection occurs in less than 1 percent of cases as an early (<30 days) complication, but may
afflict as many as 5 percent of graft recipients over the longer term (Bandyk and Esses, 1994). The usual
culprit is a staphylococcal species, but many other species have been known to infect vascular grafts
(Bunt, 1983), with different complications and rates of progression (Bandyk and Esses, 1994). Although
there is some leeway in regards to the level of therapy, infections can often be fatal unless aggressive sur-
gical means are coupled with antibiotic treatment. Because residual infection is a common cause of ther-
apeutic failure, extensive debridement and graft excision with in situ or extra-anatomic prosthetic
replacement is warranted in most cases (Calligaro and Veith, 1991; Seeger, 2000). Even with aggressive