
Page 118 - Biomedical Engineering and Design Handbook Volume 2, Applications
P. 118
OVERVIEW OF CARDIOVASCULAR DEVICES 97
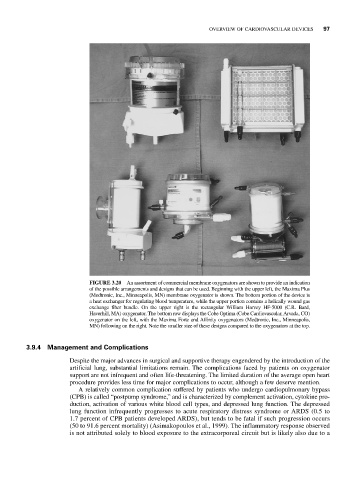
FIGURE 3.20 An assortment of commercial membrane oxygenators are shown to provide an indication
of the possible arrangements and designs that can be used. Beginning with the upper left, the Maxima Plus
(Medtronic, Inc., Minneapolis, MN) membrane oxygenator is shown. The bottom portion of the device is
a heat exchanger for regulating blood temperature, while the upper portion contains a helically wound gas
exchange fiber bundle. On the upper right is the rectangular William Harvey HF-5000 (C.R. Bard,
Haverhill, MA) oxygenator. The bottom row displays the Cobe Optima (Cobe Cardiovascular, Arvada, CO)
oxygenator on the left, with the Maxima Forte and Affinity oxygenators (Medtronic, Inc., Minneapolis,
MN) following on the right. Note the smaller size of these designs compared to the oxygenators at the top.
3.9.4 Management and Complications
Despite the major advances in surgical and supportive therapy engendered by the introduction of the
artificial lung, substantial limitations remain. The complications faced by patients on oxygenator
support are not infrequent and often life-threatening. The limited duration of the average open heart
procedure provides less time for major complications to occur, although a few deserve mention.
A relatively common complication suffered by patients who undergo cardiopulmonary bypass
(CPB) is called “postpump syndrome,” and is characterized by complement activation, cytokine pro-
duction, activation of various white blood cell types, and depressed lung function. The depressed
lung function infrequently progresses to acute respiratory distress syndrome or ARDS (0.5 to
1.7 percent of CPB patients developed ARDS), but tends to be fatal if such progression occurs
(50 to 91.6 percent mortality) (Asimakopoulos et al., 1999). The inflammatory response observed
is not attributed solely to blood exposure to the extracorporeal circuit but is likely also due to a