
Page 177 - Biomedical Engineering and Design Handbook Volume 2, Applications
P. 177
156 MEDICAL DEVICE DESIGN
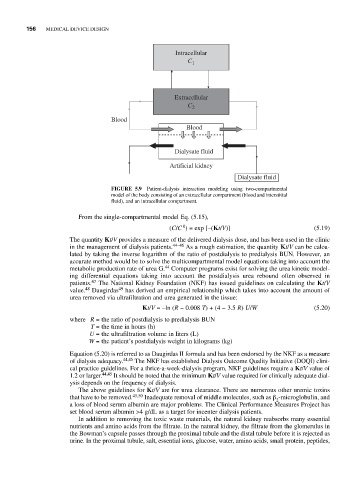
Intracellular
C 1
Extracellular
C 2
Blood
Blood
Dialysate fluid
Artificial kidney
Dialysate fluid
FIGURE 5.9 Patient-dialysis interaction modeling using two-compartmental
model of the body consisting of an extracellular compartment (blood and interstitial
fluid), and an intracellular compartment.
From the single-compartmental model Eq. (5.15),
0
(C/C ) = exp [–(Kt/V)] (5.19)
The quantity Kt/V provides a measure of the delivered dialysis dose, and has been used in the clinic
in the management of dialysis patients. 44–46 As a rough estimation, the quantity Kt/V can be calcu-
lated by taking the inverse logarithm of the ratio of postdialysis to predialysis BUN. However, an
accurate method would be to solve the multicompartmental model equations taking into account the
44
metabolic production rate of urea G. Computer programs exist for solving the urea kinetic model-
ing differential equations taking into account the postdialysis urea rebound often observed in
patients. 47 The National Kidney Foundation (NKF) has issued guidelines on calculating the Kt/V
value. 48 Daugirdas 49 has derived an empirical relationship which takes into account the amount of
urea removed via ultrafiltration and urea generated in the tissue:
Kt/V = –ln (R − 0.008 T) + (4 − 3.5 R) U/W (5.20)
where R = the ratio of postdialysis to predialysis BUN
T = the time in hours (h)
U = the ultrafiltration volume in liters (L)
W = the patient’s postdialysis weight in kilograms (kg)
Equation (5.20) is referred to as Daugirdas II formula and has been endorsed by the NKF as a measure
of dialysis adequacy. 44,45 The NKF has established Dialysis Outcome Quality Initiative (DOQI) clini-
cal practice guidelines. For a thrice-a-week-dialysis program, NKF guidelines require a Kt/V value of
1.2 or larger. 44,45 It should be noted that the minimum Kt/V value required for clinically adequate dial-
ysis depends on the frequency of dialysis.
The above guidelines for Kt/V are for urea clearance. There are numerous other uremic toxins
that have to be removed. 45,50 Inadequate removal of middle molecules, such as β -microglobulin, and
2
a loss of blood serum albumin are major problems. The Clinical Performance Measures Project has
set blood serum albumin >4 g/dL as a target for incenter dialysis patients.
In addition to removing the toxic waste materials, the natural kidney reabsorbs many essential
nutrients and amino acids from the filtrate. In the natural kidney, the filtrate from the glomerulus in
the Bowman’s capsule passes through the proximal tubule and the distal tubule before it is rejected as
urine. In the proximal tubule, salt, essential ions, glucose, water, amino acids, small protein, peptides,