
Page 453 - Handbook of Biomechatronics
P. 453
The Artificial Pancreas 447
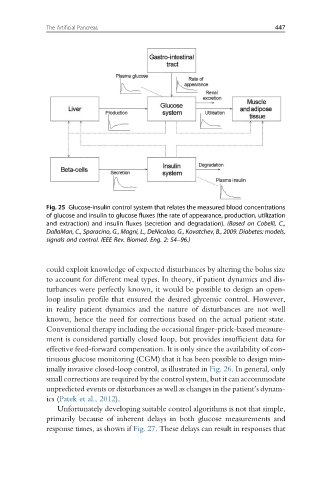
Fig. 25 Glucose-insulin control system that relates the measured blood concentrations
of glucose and insulin to glucose fluxes (the rate of appearance, production, utilization
and extraction) and insulin fluxes (secretion and degradation). (Based on Cobelli, C.,
DallaMan, C., Sparacino, G., Magni, L., DeNicolao, G., Kovatchev, B., 2009. Diabetes: models,
signals and control. IEEE Rev. Biomed. Eng. 2: 54–96.)
could exploit knowledge of expected disturbances by altering the bolus size
to account for different meal types. In theory, if patient dynamics and dis-
turbances were perfectly known, it would be possible to design an open-
loop insulin profile that ensured the desired glycemic control. However,
in reality patient dynamics and the nature of disturbances are not well
known, hence the need for corrections based on the actual patient state.
Conventional therapy including the occasional finger-prick-based measure-
ment is considered partially closed loop, but provides insufficient data for
effective feed-forward compensation. It is only since the availability of con-
tinuous glucose monitoring (CGM) that it has been possible to design min-
imally invasive closed-loop control, as illustrated in Fig. 26. In general, only
small corrections are required by the control system, but it can accommodate
unpredicted events or disturbances as well as changes in the patient’s dynam-
ics (Patek et al., 2012).
Unfortunately developing suitable control algorithms is not that simple,
primarily because of inherent delays in both glucose measurements and
response times, as shown if Fig. 27. These delays can result in responses that