
Page 419 - Biomedical Engineering and Design Handbook Volume 2, Applications
P. 419
COMPUTER-INTEGRATED SURGERY AND MEDICAL ROBOTICS 397
from the computer. The modeling and analysis processes within the computer will often rely upon
databases of prior information, such as anatomical atlases, implant design data, or descriptions of
common surgical tasks. The computer can also retain nearly all information developed during surgi-
cal planning and execution, and store it for postoperative analysis and comparison with long-term
outcomes.
Essential elements of CIS systems are devices and techniques to provide the interfaces between
the “virtual reality” of computer models and surgical plans to the “actual reality” of the operating
room, patients, and surgeons. Broadly speaking, we identify three interrelated categories of inter-
face technology: (1) imaging and sensory devices, (2) robotic devices and systems, and (3) human-
machine interfaces. Research in these areas draws on a broad spectrum of core engineering
research disciplines, such as materials science, mechanical engineering, control theory, and device
physics. The fundamental challenge is to extend the sensory, motor, and human-adaptation abili-
ties of computer-based systems in a demanding and constrained environment. Particular needs
include compactness, precision, biocompatibility, imager compatibility, dexterity, sterility, and
human factors.
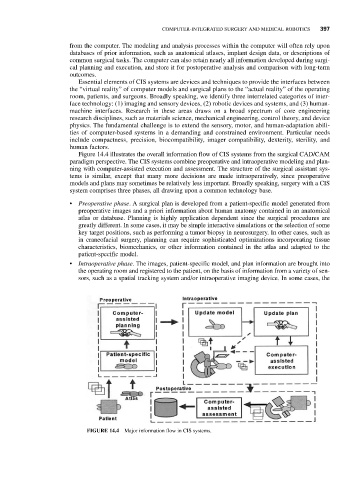
Figure 14.4 illustrates the overall information flow of CIS systems from the surgical CAD/CAM
paradigm perspective. The CIS systems combine preoperative and intraoperative modeling and plan-
ning with computer-assisted execution and assessment. The structure of the surgical assistant sys-
tems is similar, except that many more decisions are made intraoperatively, since preoperative
models and plans may sometimes be relatively less important. Broadly speaking, surgery with a CIS
system comprises three phases, all drawing upon a common technology base.
• Preoperative phase. A surgical plan is developed from a patient-specific model generated from
preoperative images and a priori information about human anatomy contained in an anatomical
atlas or database. Planning is highly application dependent since the surgical procedures are
greatly different. In some cases, it may be simple interactive simulations or the selection of some
key target positions, such as performing a tumor biopsy in neurosurgery. In other cases, such as
in craneofacial surgery, planning can require sophisticated optimizations incorporating tissue
characteristics, biomechanics, or other information contained in the atlas and adapted to the
patient-specific model.
• Intraoperative phase. The images, patient-specific model, and plan information are brought into
the operating room and registered to the patient, on the basis of information from a variety of sen-
sors, such as a spatial tracking system and/or intraoperative imaging device. In some cases, the
FIGURE 14.4 Major information flow in CIS systems.